



Colloid cyst constitutes 2% of glial tumors of ependymal origin. Postulated precursors include choroid plexus, ventricular ependymoma , the tela choroidea and the paraphysis.
Pathology : Gross: smooth spherical well delineated cystic mass of variable size filled with gelatinous material
Microscopic : collagen/ fibrous capsule lined by cuboidal/columnar epithelium.
Age and gender : Young adults 20 -40 yrs. M>F.
Location : exclusively arising from inferior aspect of septum pellucidum protruding into anterior portion of 3rd ventricle.
Clinical presentation : Colloid cysts rarely become symptomatic before age 20. Presents with positional , intermittent headaches ( transient obstruction secondary to ball valve mechanism at foramen of Monroe. Gait apraxia, change in mental status , dementia , papilledema are because of increased intracranial pressure.
Imaging :
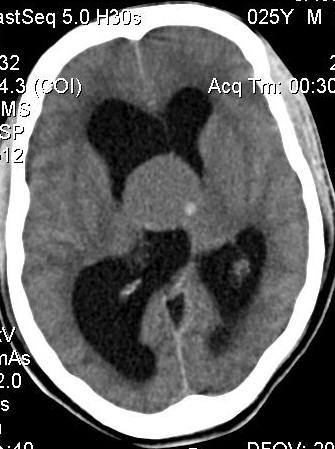
CT : 2/3rd colloid cysts are homogenously hyperdense on NECT , 1/3rd are isodense. A well delineated round or ovoid non calcified mass at foramen of Monroe is characteristic. There is no enhancement following contrast administration.
CT : 2/3rd colloid cysts are homogenously hyperdense on NECT , 1/3rd are isodense. A well delineated round or ovoid non calcified mass at foramen of Monroe is characteristic. There is no enhancement following contrast administration.
MR : The signal characteristics of colloid cysts vary widely. The most common appearance is a mass that is hyperintense on T1 and hypointense on T2 .However, they can display virtually any signal intensity on any pulse sequence . CSF flow artifacts at the foramen of Monroe can mimic colloid cyst.
Differentials : Adults : Subependymoma
Central neurocytoma
Tortuous basilar artery /aneurysm
CSF flow artifacts
Extrinsic compression ( eg. Pituitary adenoma)
Children : Germinoma
Subependymal giant cell astrocytoma
Pilocytic astrocytoma (hypothalamus)
Craniopharyngioma (suprasellar mass)
Choroid plexus papilloma(rare)